Okay, so today I want to shift focus from cardiology to developmental biology. Many people struggle to understand this subject, but in breaking it down this field can make more sense. I will divide it into segments, therefore allowing each post to offer up enough focus without getting overly complicated. If you have questions, or wish to comment, you can either send me an email or leave a comment here.
Now to the post, beginning broad and going from there...
The terms to describe the periods of development seem a lot less interesting than you'd expect. I have listed them in order, with appropriate descriptions:
- Capacitation: does the sperm have the capacity to fertilize the egg?
- Requires around 6-7 hours of sperm within vicinity of egg
- Fertilization: the sperm penetrates the egg
- Cleavages: the first two cell divisions of the fertilized egg
- Morula: a solid mass of around 16 cells
- Blastocyst: a round clump of cells with an inner liquid-filled space; the beginning of cell differentiation
Okay, thus far not so bad. You need a sperm to fertilize an egg, which will then begin to divide and grow. It all takes time, and fits well on a time line:
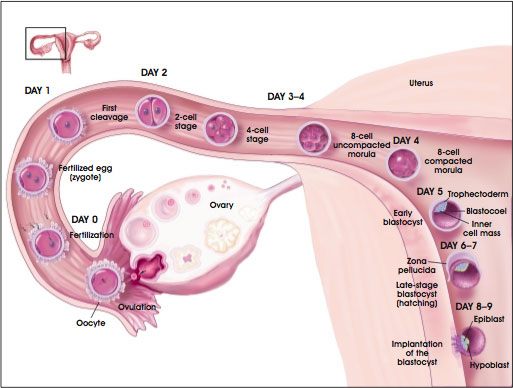
- Day 0: fertilization takes place, usually in the upper fallopian tube
- Day 3: the morula descends down the fallopian tube
- Day 4: the morula enters the uterus
- Day 5: the morula becomes a blastocyst
- Day 6: the blastocyst begins to implant into the wall of the uterus
- Day 10: implantation completes
This image, while somewhat detailed, depicts the timeline as the egg travels from the ovary, through the fallopian tube, to the uterus.
All of this assumes a normal sequence, beginning with ovulation and ending in implantation in the uterus. When something goes awry, with can think of it as an ectopic implantation--not in the upper uterus. In order of most common to least common:
- The fallopian tube: accounts for 95% of all ectopic pregnancies, it cannot grow like the uterus and will burst
- Lower uterus/cervix: can be carried to term with careful following, placenta can implant over cervix and risks tearing
- Abdominal cavity: the fertilized egg will implant to live off of the mesenteric blood supply, can be carried to term but only deliverable through c-section
- The opposite fallopian tube
Ectopic pregnancies carry significant risk to the mother, since only the uterus serves for the place in which a baby should grow. This does not mean that some ectopic pregnancies cannot end with delivery, but not all will have such an outcome. The answer to the question of how to handle an ectopic pregnancy: carried to term vs. aborted, carries significant ethical and legal implications. To anyone going into the field I strongly suggest an understanding of this topic.
Dickens, B. (2003). Ectopic pregnancy and emergency care: ethical and legal issues International Journal of Gynecology & Obstetrics, 82 (1), 121-126 DOI: 10.1016/S0020-7292(03)00175-9